|
| T1 sagittal |
 |
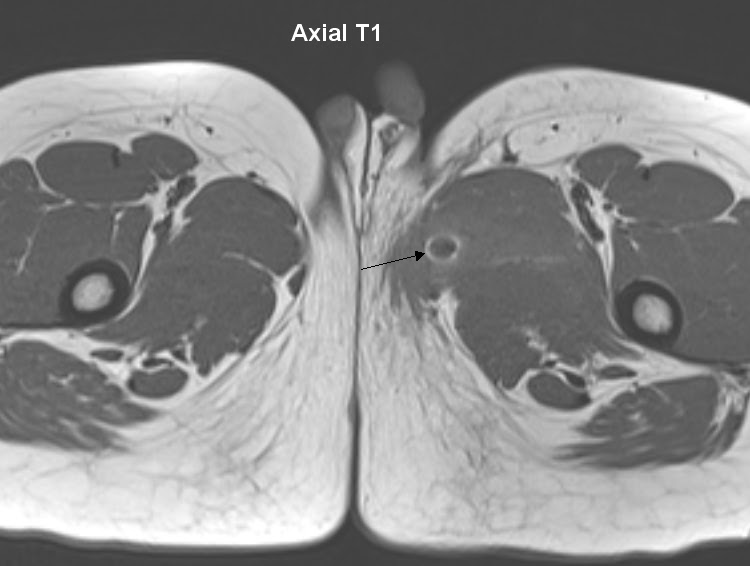
| T2 axial |
 |
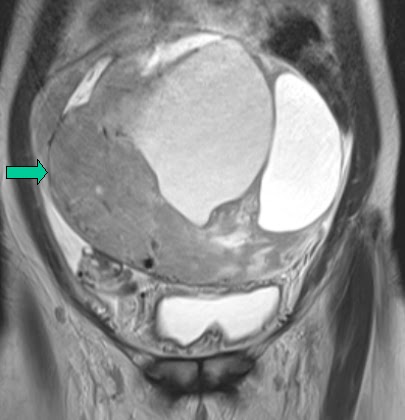
| T2 coronal |
 |
| T2 sagittal |
30 year old presented with dysuria and occassional hematuria.
MRI of the pelvis demonstrated:
- a well defined hyperintense cystic lesion on T1 and T2
- Lesion lies in the midline in close approximation to the bulbous urethra and just below the prostate.
Diagnosis: Cowper's duct cyst.
Cowper's duct cyst:
- Cowpers glands - found in the urogenital diaphragm below the prostate
- Drains into the bulbar urethra
- Obstruction results in retention cysts
- Cowper's gland cysts are probably secondary to trauma or infection
- Large cysts can cause urinary obstruction, hematuria or infertility.
- Treated by marsupialisation or endoscopic incision.
References:
http://www.ajronline.org/doi/full/10.2214/AJR.06.0759
http://link.springer.com/article/10.1007%2Fs00247-001-0580-8
http://link.springer.com/article/10.1007%2Fs00247-001-0580-8